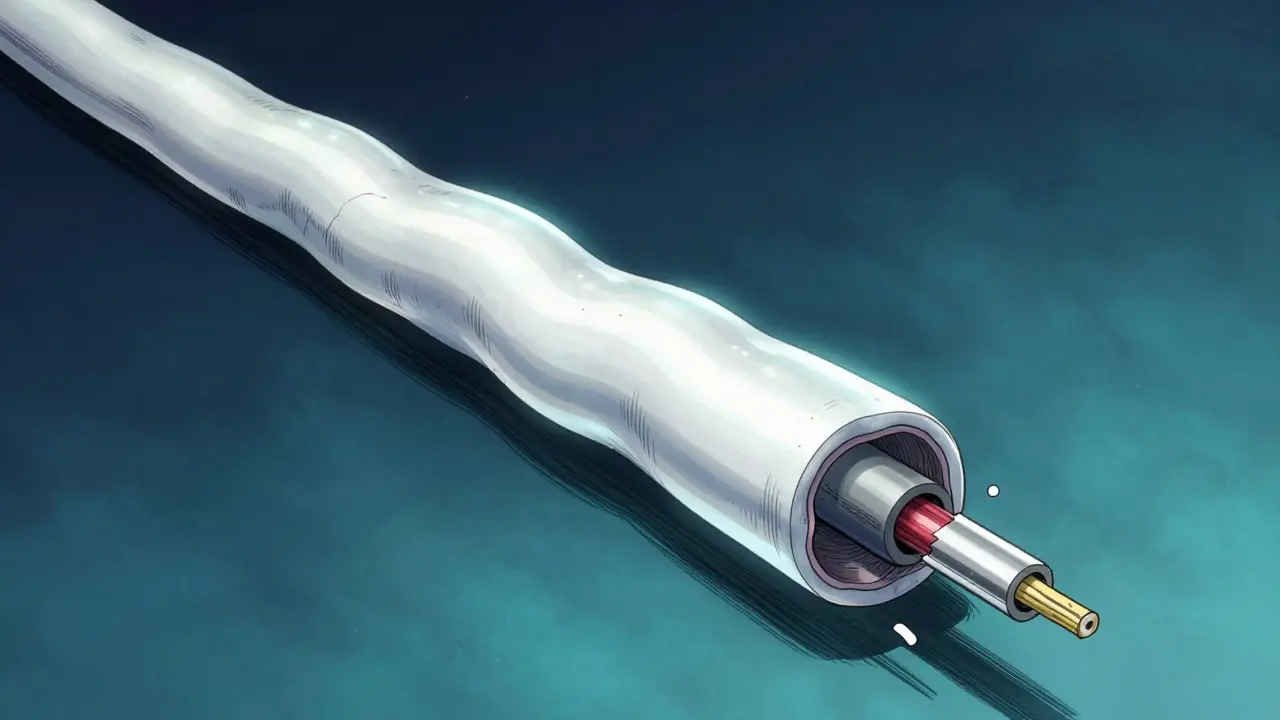
Imagine your nerves are like electrical wires. To keep the signal moving fast and clear, these wires are wrapped in an insulating layer called myelin. Now, imagine that insulation is being stripped away. That is essentially what happens with Multiple Sclerosis is a chronic autoimmune disorder where the body's immune system attacks the protective sheath that covers nerve fibers in the central nervous system. When this happens, the "messages" from your brain get garbled, slowed down, or stopped entirely.
For many, this starts as a series of unpredictable attacks-sudden bouts of blurred vision or tingling limbs that eventually fade. But for others, the challenge isn't just these spikes in symptoms; it's a slow, steady decline in function. Understanding why some people stay stable while others experience steady neurological deterioration is the key to modern treatment strategies. While we have many tools to stop the "attacks," protecting the actual nerve fibers remains the great frontier of MS research.
The Different Faces of MS
MS doesn't look the same for everyone. Depending on how the disease progresses, doctors categorize it into a few primary forms. Most people start with Relapsing-Remitting MS (RRMS), which accounts for about 85% of initial diagnoses. In this stage, you have clear relapses followed by periods of partial or complete recovery. However, over time, many of these patients transition into Secondary Progressive MS (SPMS), where the decline becomes more gradual and constant.
Then there is Primary Progressive MS (PPMS). Unlike the relapsing form, PPMS doesn't have those clear "up and down" periods. Instead, it's a steady decline from the very start. The danger here is that because there aren't dramatic relapses, the damage can accumulate silently before it's fully recognized.
| Subtype | Pattern of Progression | Initial Prevalence | Primary Driver |
|---|---|---|---|
| RRMS | Relapses followed by remission | ~85% | Peripheral immune response |
| SPMS | Steady decline after initial relapses | Transitions from RRMS | CNS-internal immune reactions |
| PPMS | Gradual decline from onset | ~15% | Diffuse axonal degeneration |
Why the Brain Deteriorates: Demyelination vs. Axonal Loss
It's important to distinguish between losing the "insulation" and losing the "wire" itself. When the immune system attacks the myelin, it causes inflammation and edema (swelling). This swelling can block nerve signals, causing a sudden relapse. The good news? Demyelination is often reversible. The brain can sometimes repair the myelin or find a way to route signals around the damaged spot.
The real problem is axonal degeneration. When the Axon-the actual fiber of the nerve cell-is severed or destroyed, the loss is usually permanent. Research has shown that in chronic MS, about 50% of these fibers in spinal lesions show fragmented structures and a massive drop in mitochondria (the cell's power plants). Without energy and a physical path, the signal simply cannot get through.
This is why some patients continue to get worse even when their MRI doesn't show any new "spots" or lesions. The inflammation might be gone, but the underlying neurons are starving or dying off. This process is often driven by mitochondrial failure and the loss of specific receptors, like the astrocytic β2-adrenergic receptors, which normally help protect the nerves from injury.
How Disease-Modifying Therapies (DMTs) Work
Disease-Modifying Therapy (DMT) is the cornerstone of MS management. Unlike steroids, which treat the symptoms of a current attack, DMTs aim to change the course of the disease. As of 2023, there are over 20 FDA-approved medications designed to reduce the frequency and severity of relapses.
Most current DMTs focus on the "border patrol." They stop aggressive immune cells from crossing the blood-brain barrier into the central nervous system. For people with RRMS, this is incredibly effective, often reducing relapse rates by 30% to 50%. By stopping the fire (inflammation), they prevent the creation of new lesions.
However, there's a catch: most current DMTs are not great at stopping the slow, "smoldering" progression seen in SPMS or PPMS. In these advanced stages, the immune reaction is already inside the brain, often involving B cells forming follicle-like structures in the meninges (the brain's lining). Because the damage is now more about neurodegeneration than active inflammation, traditional anti-inflammatories have limited impact.
The Future: Moving Toward Neuroprotection
Since we can't rely solely on anti-inflammatories to stop progressive decline, the focus is shifting toward neuroprotection and remyelination. The goal is to keep the axons alive even if the myelin is gone, or better yet, grow the myelin back.
Scientists have identified specific "brake" proteins-like Nogo and LINGO-1-that naturally prevent nerves from regenerating in the adult brain. By blocking these inhibitors, researchers hope to unlock the brain's ability to repair itself. There are currently numerous phase II and III clinical trials focusing on:
- Mitochondrial Support: Trying to restore the energy supply to struggling axons to prevent them from dying.
- Sodium Channel Modulation: Adjusting how ions move across the nerve membrane to keep signals flowing despite demyelination.
- Remyelination Strategies: Encouraging oligodendrocytes (the cells that make myelin) to wrap new insulation around bare nerves.

Monitoring Progression: Beyond the MRI
For years, the MRI was the gold standard. If you didn't see a new lesion, you were "stable." But we now know that brain atrophy-the actual shrinking of the gray and white matter-is a better predictor of long-term disability. Specifically, gray matter atrophy often correlates more closely with a patient's actual functional ability than the number of white matter spots.
Doctors are also looking at Magnetization Transfer Ratio (MTR) imaging. This helps identify "normal-appearing white matter" that looks fine on a standard scan but is actually suffering from microglial activation and early axonal decay. It's like finding a leak in a pipe before the whole wall collapses.
Can MS be cured?
Currently, there is no cure for MS. However, Disease-Modifying Therapies (DMTs) can significantly slow the progression of the disease, reduce the number of relapses, and improve the quality of life by preventing further neurological damage.
What is the difference between a relapse and progression?
A relapse is a sudden attack of new or worsening neurological symptoms caused by active inflammation. Progression is a gradual decline in function over months or years, often caused by axonal degeneration and the cumulative loss of neurons, even without new inflammatory activity.
Why do some people transition from RRMS to SPMS?
About 40% of patients transition within 10-15 years. This typically happens because chronically demyelinated axons eventually fail and die. As the brain's ability to compensate for this damage wears thin, the disease moves from a relapsing pattern to a steady decline.
Do lifestyle factors impact MS?
Yes. Research indicates that environmental triggers such as low vitamin D levels, smoking, and exposure to the Epstein-Barr virus can play a role in the onset and progression of the disease, interacting with a person's genetic susceptibility.
Are all DMTs the same?
No. Some DMTs are injectables that modulate the immune system, while others are monoclonal antibodies (infusions) that target specific B cells or T cells. The choice depends on the subtype of MS, the severity of the disease, and the patient's overall health.
Next Steps for Management
If you or a loved one is navigating an MS diagnosis, the most important thing is early intervention. Starting a high-efficacy DMT during the relapsing-remitting phase can potentially delay the transition to progressive MS by years. Focus on a multidisciplinary approach: pair your neurologist's medication plan with physical therapy to maintain mobility and cognitive exercises to build "brain reserve." If you notice a steady decline in function despite a "clean" MRI, talk to your specialist about newer imaging techniques or clinical trials focusing on neuroprotection.





