
When efavirenz stops working, it’s not just a bad day-it’s a medical turning point. For people living with HIV, efavirenz has been a backbone of treatment for over two decades. But if the virus starts multiplying again despite taking the drug, resistance has likely kicked in. And that’s not something you can ignore. This isn’t about missing a pill now and then. This is about the virus changing its shape to survive the very medicine meant to kill it.
How Efavirenz Resistance Starts
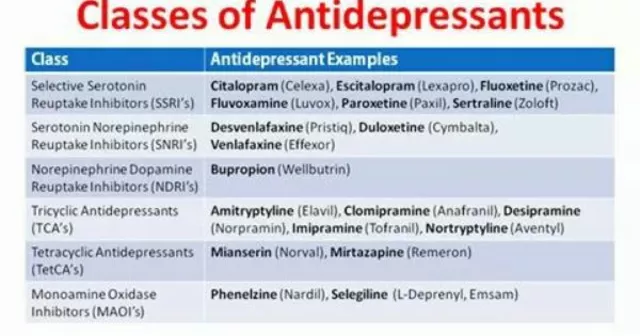
Efavirenz belongs to a class of drugs called non-nucleoside reverse transcriptase inhibitors (NNRTIs). It works by blocking HIV’s reverse transcriptase enzyme-the tool the virus uses to copy its RNA into DNA so it can take over your cells. But HIV is a master of mutation. Every time it copies itself, it makes mistakes. Most of those mistakes kill the virus. But sometimes, one of those mistakes gives the virus a shield against efavirenz.
The most common mutation linked to efavirenz resistance is K103N. This single change in the virus’s genetic code makes efavirenz unable to bind properly. Once that mutation is in place, the drug loses most of its power. Studies show that up to 80% of people who develop efavirenz resistance have this exact mutation. It doesn’t take years. It can happen in weeks if the drug level in your blood drops too low.
Low drug levels? That’s usually the real trigger. Skipping doses, taking efavirenz with food that interferes with absorption (like high-fat meals), or mixing it with other meds that speed up liver breakdown-all of these can lower the concentration of efavirenz in your bloodstream. When the drug level dips below the threshold needed to suppress the virus, even for a few hours, resistant strains get a chance to grow.
Who’s Most at Risk
Not everyone on efavirenz develops resistance. But some groups are more vulnerable. People with low baseline CD4 counts-under 200 cells/mm³-when they start treatment are at higher risk. Why? Their viral load is already high, meaning more virus copies = more chances for mutations to occur.
People who start efavirenz without first testing for pre-existing resistance are also at risk. In some regions, up to 15% of new HIV cases already carry NNRTI-resistant strains. If you’re given efavirenz without knowing that, you’re starting a battle you’re already losing.
And then there’s adherence. If you miss more than one or two doses a month, your risk of resistance jumps significantly. Efavirenz has a long half-life, so it sticks around in your body longer than many other HIV drugs. That’s a double-edged sword: it allows for once-daily dosing, but it also means that when you skip a dose, the drug level doesn’t crash immediately. That gives the virus a slow, quiet window to adapt.
How to Spot Resistance Early
Resistance doesn’t come with a warning label. You won’t feel sick because of it. The only way to know is through regular testing.
- Every 3 to 6 months, get a viral load test. If your viral load, which was previously undetectable, rises above 200 copies/mL, resistance is a strong possibility.
- If your viral load stays above 1,000 copies/mL for more than 2 months, resistance is very likely.
- Resistance testing (genotypic testing) should follow any confirmed viral rebound. This test looks at the virus’s genetic code to find known resistance mutations like K103N, Y181C, or G190A.
Don’t wait for symptoms. Fatigue, fever, or night sweats might mean something else entirely-like a cold or stress. HIV resistance is silent until it’s advanced.

Solutions: What to Do When Efavirenz Fails
If resistance is confirmed, switching treatment is not optional. You can’t fix it with more efavirenz. You need a new combination.
The first step is to choose a new backbone. Dolutegravir is now the go-to for most people who fail efavirenz. It’s an integrase inhibitor, works differently, and has a high barrier to resistance. Even if you have multiple drug resistances, dolutegravir often still works.
Other options include:
- Elvitegravir/cobicistat/emtricitabine/tenofovir (Stribild)
- Bictegravir/emtricitabine/tenofovir alafenamide (Biktarvy)
- Rilpivirine (if no prior NNRTI resistance and viral load is under 100,000)
Never switch just one drug. That’s like replacing one soldier in a losing army-it won’t turn the tide. You need a full new combo, usually two or three drugs from different classes.
For people with complex resistance, newer drugs like fostemsavir or ibalizumab may be options. These are reserved for cases where most drugs have failed, but they’re life-changing when used correctly.
Preventing Resistance Before It Starts
The best solution is to never let resistance develop in the first place.
- Always test for resistance before starting any HIV regimen. This is standard in most high-income countries but still skipped in many low-resource settings. Push for it.
- Take efavirenz on an empty stomach, or with a light meal. High-fat meals can spike drug absorption unpredictably.
- Use pill organizers and phone alarms. Set reminders for the same time every day-even if you feel fine.
- Don’t mix efavirenz with herbal supplements like St. John’s Wort. It can drop efavirenz levels by 50% or more.
- Ask your doctor about drug interactions. Antibiotics, antifungals, and even some acid reducers can interfere.
Also, consider switching to a newer regimen if you’re stable. Efavirenz is being phased out in many countries because of its side effects-dizziness, nightmares, mood changes-and the availability of better-tolerated drugs. If you’re doing well on efavirenz but have no resistance, switching to dolutegravir or bictegravir might be worth discussing. Fewer side effects + higher barrier to resistance = better long-term outcomes.
What Happens If You Don’t Act
Ignoring resistance doesn’t mean the virus goes away. It means it keeps evolving. Each new mutation makes your options smaller. You might end up with a virus that’s resistant to most NNRTIs, some NRTIs, and even a few protease inhibitors. That’s called multi-drug resistance.
Once you hit that point, treatment becomes harder, more expensive, and often involves injections or infusions. Your risk of developing AIDS-related illnesses rises. Your life expectancy drops. And worse-you can pass on a resistant strain to someone else.
Resistant HIV isn’t just your problem. It’s a public health issue.
Real-World Example
In a 2024 study from South Africa, 42% of patients who failed efavirenz-based treatment had the K103N mutation. Most of them had missed doses due to stigma, transportation issues, or not understanding the importance of consistency. After switching to dolutegravir-based regimens, 94% achieved viral suppression within 6 months. The fix wasn’t magic. It was consistency, testing, and the right next drug.
This isn’t theoretical. It’s happening right now-in clinics, homes, and communities around the world.
Bottom Line
Efavirenz resistance is preventable. It’s treatable. But it’s not ignorable. If you’re on efavirenz, get tested regularly. Take your pills on time. Talk to your doctor about alternatives. Don’t wait for symptoms. Don’t assume you’re fine because you feel okay. HIV doesn’t care how you feel. It only cares if the drug level drops-even for a few hours.
Your health isn’t just about taking a pill. It’s about understanding what happens when that pill stops working-and what to do next.
Can efavirenz resistance be reversed?
No, once the virus develops resistance mutations like K103N, those changes are permanent in that strain. You can’t undo the mutation. But you can stop the resistant virus from spreading by switching to a new drug regimen that still works. The resistant strain may fade over time if it’s not being selected for, but it can come back if you go back on efavirenz.
Is efavirenz still used today?
Yes, but less often. Many countries have moved to dolutegravir or bictegravir as first-line treatments because they’re more effective, have fewer side effects, and are harder for the virus to resist. Efavirenz is still used in some low-income regions because it’s cheaper, but it’s no longer the preferred choice in most guidelines.
Can I take efavirenz with alcohol?
Moderate alcohol use is generally safe, but heavy drinking increases the risk of liver damage and can interfere with your ability to take the drug consistently. Efavirenz is processed by the liver, and alcohol adds stress. If you drink regularly, talk to your doctor about liver monitoring.
How long does it take for resistance to develop?
It can happen in as little as 2-4 weeks if drug levels are consistently low due to missed doses or interactions. But it can also take months or years if you’re perfectly adherent. The speed depends on how often the virus gets a chance to replicate under drug pressure.
Will I need to take HIV meds for life if I develop resistance?
Yes. Even if you switch to a new regimen and suppress the virus again, you’ll still need to take HIV medication daily for life. Resistance doesn’t mean you’re cured-it means you’ve learned what doesn’t work. You still need treatment to stay healthy and prevent transmission.





Dale Yu
October 27, 2025 AT 17:19Stop lying to yourself if you think skipping a pill is no big deal
May Zone skelah
October 27, 2025 AT 23:52Let me tell you something about efavirenz resistance that the medical journals won't tell you - it's not just about the K103N mutation, it's about systemic neglect. People in rural areas don't have access to consistent refrigeration for their meds, let alone the luxury of a pill organizer. The real villain isn't the virus, it's the healthcare infrastructure that treats HIV like a chronic inconvenience instead of a life-or-death emergency. I've seen patients go months without testing because the nearest clinic is two states away and they work two jobs just to afford bus fare. Resistance isn't a failure of adherence - it's a failure of society. And now we're supposed to act shocked when the virus evolves faster than our compassion? The fact that we still use efavirenz in low-income countries because it's cheap is a moral crime disguised as public health policy.
Kshitij Nim
October 29, 2025 AT 04:40Good breakdown. I work in a clinic in Mumbai and we switched 80% of our efavirenz patients to dolutegravir last year. Side effects dropped, viral loads plummeted. The key? Daily reminders via WhatsApp. No fancy tech - just simple texts. People respond to consistency, not lectures.
Scott Horvath
October 30, 2025 AT 12:24man i was on efavirenz for 3 years and honestly the nightmares were wild like i'd wake up screaming thinking i was being chased by a giant condom
switched to biktarvy and now i sleep like a baby
also no more dizziness when i stand up
if you still on efavirenz and feel fine just know your body is lying to you
Armando Rodriguez
October 31, 2025 AT 20:21Thank you for this comprehensive and clinically accurate overview. The emphasis on early viral load monitoring is critical, as is the recommendation against monotherapy switches. These principles align with current CDC and WHO guidelines and underscore the importance of patient education in sustaining long-term virologic suppression. I encourage all providers to integrate resistance testing into routine care protocols.
jennifer sizemore
November 1, 2025 AT 00:58I’ve been on HIV meds for 15 years and I can say this: the hardest part isn’t the pills - it’s the silence. No one talks about how scary it is to miss a dose and wonder if you’re becoming a statistic. But we’re all in this together. If you’re reading this and you’re struggling - you’re not alone. Reach out. Talk to someone. Your health matters more than your shame.
matt tricarico
November 1, 2025 AT 03:46Of course resistance happens. People are lazy. They don’t want to be reminded they’re sick. They’d rather blame the drug than their own inability to follow basic instructions. This isn’t rocket science. Take the pill. Don’t eat fatty food. Don’t mix with St. John’s Wort. Simple. But no - they need a 2000-word essay to understand why they can’t be irresponsible.
Kimberly Ford
November 1, 2025 AT 21:46For anyone reading this who’s scared to switch meds - I get it. Change is terrifying. But I switched from efavirenz to bictegravir after 7 years and my mental clarity improved instantly. No more zombie mode at work. No more crying for no reason. The science is clear: newer regimens are safer, simpler, and more forgiving. Don’t wait until you’re in crisis to ask for an upgrade. You deserve better than a drug from the 2000s.
jerry woo
November 2, 2025 AT 19:17efavirenz is the HIV equivalent of a flip phone in 2024 - functional, sure, but why the hell are you still using it? The virus isn’t stupid - it’s outsmarting us because we’re clinging to relics. Dolutegravir doesn’t just work better - it laughs in the face of K103N like it’s a bad meme. And if you’re still on efavirenz because you ‘can’t afford’ the new stuff - then you’re not poor, you’re just being exploited by a broken system. Fight for your meds. Your liver will thank you.
Jillian Fisher
November 3, 2025 AT 23:30i’ve been on efavirenz since 2020 and i’ve never missed a dose but my viral load spiked last month… i’m getting tested next week but i’m terrified. is it possible to have resistance even with perfect adherence? i read about drug interactions but i don’t take anything else…
Rachel Marco-Havens
November 5, 2025 AT 16:09People who miss doses are selfish. They don’t think about the fact that their resistance could spread to their partner, their kids, their community. This isn’t just about you - it’s about the entire HIV epidemic. If you can’t be responsible enough to take your pills, you shouldn’t be allowed to have sex. Period.
Kathryn Conant
November 7, 2025 AT 03:39THIS. IS. LIFE. OR DEATH. Not a suggestion. Not a recommendation. A goddamn imperative. If you’re on efavirenz and you’re not getting tested every 3 months - you’re playing Russian roulette with your future. And if you’re in a region where testing is hard - organize. Advocate. Demand change. Your life is not a footnote in a global health report. You are worth more than cheap drugs and broken systems. Rise up.